Why SERMs Have Such a High Status?
Abstract
SERMs are a group of drugs that selectively target the estrogen receptor in the body. Their unique mechanism of action allows them to act as either estrogen agonists or antagonists depending on the tissue they are acting on. This makes them versatile and useful for a variety of medical purposes. They are commonly used in the treatment of breast cancer, prevention and treatment of osteoporosis, and hormone replacement therapy for menopausal women. SERMs such as tamoxifen, raloxifene, and toremifene are well-known examples of this drug class. Though they can have side effects, they are generally well-tolerated and offer many benefits to patients.
What are SERMs?
Selective estrogen receptor modulators ( SERMs ) are a class of non-steroidal compounds that bind to estrogen receptors ( ERs ). Depending on the target tissue and the internal environment of the hormone, they are manifested as estrogen agonists and/or estrogen antagonists. According to the chemical structure, SERMs are divided into five categories: 1 triphenylethylene ccompound2 benzothiophene compounds ; 3 Naphthalene compounds; 4 benzopyran compounds 5 Other compounds.
Characteristics of SERM
SERM is a synthetic non-steroidal compound that can selectively bind to estrogen receptors in different parts and tissues of the body, showing different physiological effects. It binds to estrogen receptors of osteoclasts and the cardiovascular system ( vascular endothelial cells ), exhibits estrogenic effects, inhibits osteoclast-mediated bone resorption, and reduces serum cholesterol and low-density lipoprotein. It binds to estrogen receptors in the mammary gland ( breast cells ) and endometrial sites ( epithelial and myometrial cells, etc. ), showing anti-estrogen effects and inhibiting the proliferation of endometrial epithelial cells in breast cells.
Classification of SERM
( 1 ) Triphenylethylene compounds: estrogen agonists and estrogen antagonists.
1 ) Tamoxifen ( TAM ) is a derivative of triphenylethylene. TAM is the earliest synthetic SERM and the representative compound of the first-generation SERMs. It is used to treat ER-positive advanced breast cancer and is still an adjuvant therapy for breast cancer. The selective regulation of tamoxifen on ER is as follows: it is an ER antagonist for breast tissue and an ER agonist for bone tissue, the cardiovascular system, and the uterus. It can selectively bind to estrogen receptors on bone cells to inhibit bone loss and show the nti-estrogen effect on breast cells, so it is used in the treatment of breast cancer. However, TAM has estrogen-like effects on the endometrium, and long-term application may lead to endometrial hyperplasia. Therefore, the clinical application of TAM, especially in the prevention and treatment of osteoporosis in postmenopausal women, is limited.
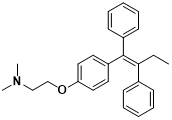
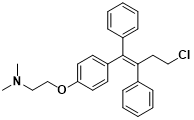
Triphenoxyamine structure formula Toremifene structural formula
2 ) Toremifene and tamoxifen have similar clinical efficacy and adverse reactions. The difference is that toremifene can increase high-density lipoprotein and has a less estrogen-like effect on bone tissue than tamoxifen.
3 ) Tamoxifen derivatives : miproxifen and idoxifen. Miproxifene is used to treat ER-related breast cancer. Idoxifene is a preventive and therapeutic drug for osteoporosis in postmenopausal women. The side effects were dose-related, manifested as hot flashes, abnormal leucorrhea, and endometrial thickening.
( 2 ) Benzothiophene compounds: prevention and treatment of postmenopausal osteoporosis
Raloxifene hydrochloride ( RAL ) is the second generation of SERMs, which is commonly used to prevent and treat postmenopausal osteoporosis, hyperlipidemia, menopausal syndrome, and breast cancer without increasing the risk of endometrial cancer.
RAL and its analogs have antagonistic estrogenic effects on the breast and uterus, and estrogenic effects on the bone and cardiovascular system. These drugs meet the needs of postmenopausal women for estrogen in the prevention and treatment of osteoporosis while avoiding the possible side effects of estrogen. The common adverse reactions were facial flushing and lower limb muscle pain spasm, and the serious adverse reaction was venous thromboembolism. There was no significant effect on the emotional and cognitive function of postmenopausal women. It is recommended that the oral dose is 60 mg / d, and the antagonistic effect of raloxifene hydrochloride ( Ly-32639 ) on the endometrium is similar to that of raloxifene, and clinical trials are underway.
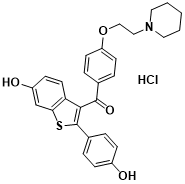
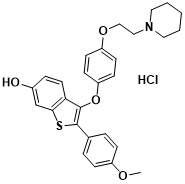
Ranoloxifene structural formula raloxifene hydrochloride structural formula
( 3 ) Naphthalenes and benzopyrans: under development
Naphthalenes CP-336156 is a third-generation SERMs compound used to treat postmenopausal women with osteoporosis, atherosclerosis, and ER-related breast cancer. Is in the phase III clinical research stage. Benzopyran compound EM-800 is a dihydro benzopyran precursor drug, and its active metabolite is EM-652. It shows that ER antagonist acts on breast tissue similar to raloxifene. It can effectively inhibit the growth of breast cancer cells, and it can block the activity of ER AF-1 and AF-2. It can be used to treat tamoxifen-resistant advanced breast cancer.
CP-336156 structural formula
Effect of SERMs
Selective estrogen receptor modulators (SERMs) are a class of compounds that interact with estrogen receptors in different tissues throughout the body. SERMs have both estrogenic and antiestrogenic effects, depending on the tissue and receptor subtype involved.
In breast tissue, SERMs act as estrogen receptor antagonists, blocking the effects of estrogen on breast cells and reducing the risk of breast cancer development in women at high risk of the disease. Tamoxifen is the most well-known and widely used SERM for breast cancer prevention and treatment. It is also used in the treatment of estrogen receptor-positive breast cancer.
In bone tissue, SERMs have estrogen-like effects and improve bone density, reducing the risk of osteoporosis and fractures. Raloxifene is a SERM approved for the prevention and treatment of osteoporosis in postmenopausal women.
SERMs can have both positive and negative effects on the cardiovascular system. Although estrogen has a protective effect on the cardiovascular system and reduces the risk of heart disease in premenopausal women, estrogen replacement therapy is associated with an increased risk of heart disease and stroke in postmenopausal women. SERMs such as raloxifene and tamoxifen have been shown to improve lipid profiles and reduce the risk of cardiovascular events in postmenopausal women with osteoporosis.
In the reproductive system, SERMs can have mixed effects. Tamoxifen can interfere with fertility in women by reducing the production of estrogen and inhibiting ovulation. However, other SERMs such as clomiphene and letrozole are used to stimulate ovulation and treat infertility in women with ovulatory disorders.
SERMs have potential applications in the prevention and treatment of various diseases, including breast cancer and osteoporosis. However, their effects on cardiovascular risk and fertility are uncertain and require further investigation.
Additionally, SERMs have shown promise in the treatment of Alzheimer’s disease, prostate cancer, and endometrial cancer. Nonetheless, additional research is required to determine their safety and effectiveness in these indications. Overall, the effects of SERMs are diverse and tissue-specific, with both potential benefits and risks.
Application of SERMs
SERMs, (selective estrogen receptor modulators)are a group of medications that are widely used to treat different conditions such as breast cancer, osteoporosis, and menopausal symptoms. The mechanism of action of SERMs is based on their ability to selectively bind to estrogen receptors in various tissues throughout the body, producing different effects depending on the tissue. One of the main applications of SERMs is in breast cancer treatment, where they can inhibit the effects of estrogen on breast tissue, thus slowing down or halting the growth of cancer cells. Moreover, SERMs can be utilized as preventive measures against the development of breast cancer in high-risk women.
Additionally, SERMs can also provide benefits in treating osteoporosis by blocking the effects of estrogen on bone tissue, thus reducing the risk of fractures in postmenopausal women. Furthermore, SERMs can alleviate menopausal symptoms such as hot flashes and vaginal dryness by selectively binding to estrogen receptors in certain tissues without increasing the risk of breast cancer.
Overall, SERMs are a versatile class of medications that can be used to treat a range of medical conditions. The efficacy of SERMs varies depending on the specific condition being treated and the individual patient’s health status and medical history. While SERMs can cause side effects, they are generally well-tolerated and can provide significant benefits for many patients.
Hormone replacement therapy (HRT)
Hormone replacement therapy (HRT) is a treatment option for women experiencing menopausal symptoms like hot flashes, vaginal dryness, and mood changes. It involves taking estrogen and sometimes progestin to replace the hormones that the body stops producing during menopause. HRT comes in various forms, allowing women to choose the best method for them. While effective in reducing menopausal symptoms and preventing bone loss and fractures, HRT has associated risks such as an increased risk of breast cancer, stroke, blood clots, and cardiovascular disease. Therefore, each woman and her healthcare provider should carefully weigh the risks and benefits of HRT. Women with breast cancer, a high risk of breast cancer, or a history of blood clots or stroke should not take HRT. Moreover, women should be aware that the full effects of HRT may take several weeks or months to be felt and should only use it for the shortest time possible. In summary, HRT is an effective treatment option, but its risks and benefits should be carefully considered by each woman and her healthcare provider.
Breast cancer treatment
Breast cancer is a prevalent type of cancer that affects women. It is characterized by the uncontrolled growth and multiplication of abnormal cells in the breast tissue. However, several effective treatment options are available for breast cancer.
Surgery is the most common treatment for breast cancer, and it aims to remove the tumor and surrounding tissues that may contain cancer cells. The type of surgery recommended may vary depending on the size and location of the tumor. A lumpectomy may be performed to remove the tumor and surrounding tissue, while a mastectomy may be recommended to remove the entire breast. Radiation therapy may also be recommended after surgery to destroy any remaining cancer cells. This type of therapy uses high-energy radiation to kill cancer cells and shrink tumors. Chemotherapy uses drugs to kill cancer cells throughout the body and may be used before or after surgery.
Hormone therapy is used for women with hormone receptor-positive breast cancer, where the cancer cells have receptors for estrogen or progesterone. This therapy works by blocking the effects of these hormones on the cancer cells, which slows or stops the growth of the tumor. Targeted therapy is a newer treatment option that targets specific proteins or genes involved in the growth and spread of cancer cells. It is usually used in combination with chemotherapy or hormone therapy.
In conclusion, the treatment of breast cancer typically involves a combination of surgery, radiation therapy, chemotherapy, hormone therapy, and targeted therapy. The specific treatment plan will depend on the stage and type of breast cancer, as well as the individual patient’s health and preferences. Early detection and appropriate treatment can increase the chances of survival and a long, healthy life for women with breast cancer.
Osteoporosis prevention and treatment
Osteoporosis is a disease characterized by reduced bone mass, increased brittleness, and increased susceptibility to fractures, especially in postmenopausal women. However, there are several ways to effectively prevent and treat osteoporosis.
The key measure to prevent osteoporosis is to ensure adequate calcium and vitamin D intake. Calcium is essential for strong bones, and vitamin D helps the body absorb calcium. A diet rich in calcium and vitamin D, with appropriate supplements, can help prevent osteoporosis. Exercise is also important for preventing osteoporosis. Weight-bearing exercises such as running, walking, and dancing can help strengthen bones and reduce the risk of fractures. Resistance exercise, such as weightlifting, can also increase bone density.
In addition to lifestyle changes, drugs can also be used to treat osteoporosis. Bisphosphonates, hormone therapy, and selective estrogen receptor modulators ( SERMs ) play a role in slowing bone loss or building new bone.
To sum up, the prevention of osteoporosis includes des healthy diet, regular expand case, avoiding smoking, and excessive drinking.
Menopause and menopausal symptoms
Menopause is a natural biological event that typically occurs between the ages of 45 and 55, signaling the end of a woman’s reproductive years. Menopause is characterized by the absence of menstrual periods for 12 consecutive months. The hormonal changes during menopause can cause a range of symptoms, such as hot flashes, night sweats, mood swings, vaginal dryness, and trouble sleeping. These symptoms are mainly caused by a decrease in estrogen and progesterone production. Fortunately, several treatment options are available for managing menopausal symptoms.
Hormone replacement therapy (HRT) involves replacing the hormones that the body stops producing during menopause, and can be effective in reducing symptoms like hot flashes and vaginal dryness. However, it is not without risks and should be carefully considered by each woman and her healthcare provider. Other non-hormonal treatment options include lifestyle modifications such as regular exercise, healthy eating, and stress-reducing techniques. Certain medications, such as selective serotonin reuptake inhibitors (SSRIs), can also help manage hot flashes and mood changes.
Estrogen receptor (ER)-positive breast cancer
ER-positive breast cancer is a prevalent type of breast cancer that is stimulated by the hormone estrogen, accounting for about 80% of all cases. This type of cancer grows slowly and responds well to hormone therapy. ER-positive breast cancer cells have receptors on their surface that bind to estrogen, which can trigger the growth and division of cancer cells. Hormone therapy helps block the effects of estrogen on these receptors, which can slow or halt the growth of the tumor.
Various hormone therapy treatments are available for the treatment of ER-positive breast cancer, such as selective estrogen receptor modulators (SERMs), aromatase inhibitors, and estrogen receptor downregulation. These treatments either hinder estrogen production or stop estrogen’s effects on cancer cells.
ER-positive breast cancer is a common type of breast cancer that depends on the hormone estrogen. Hormone therapy is a useful treatment option, and different hormone therapy treatments are available. Surgery, radiation therapy, and chemotherapy are also used in the treatment of ER-positive breast cancer.
Risks of SERMs
Selective estrogen receptor modulators are very important compounds whose main function is female sex hormones. They play different roles, ranging from maintaining mental health to maintaining the balance of water, sodium, and other substances in the body. Since maintaining health requires estrogen, its imbalance can cause health problems such as breast cancer and osteoporosis. Many forms of breast cancer depend on a stable supply of estrogen to grow and spread, while osteoporosis is usually caused by estrogen deficiency. It is common to treat these two diseases by using selective estrogen receptor modulators.
For example, Tamoxifen is a selective estrogen receptor modulator that acts as an estrogen receptor antagonist in breast tissue. Therefore, tamoxifen treatment can significantly delay the development of estrogen receptor-positive breast cancer. It works by blocking receptor sites in breast tissue ( normally activated by estrogen ). Tamoxifen also has a beneficial side effect, acting as a bone tissue agonist that can be used to fight osteoporosis by promoting increased bone density.
The use of selective estrogen receptor modulators during treatment can lead to some side effects because they act as agonists or antagonists in different parts of the human body. Although specific selective estrogen receptor modulators can prevent one cancer, they may also promote the development of another cancer. In addition, they also have an unstable impact on people’s mental health, because they affect the amount of estrogen in the body, and estrogen is important for maintaining mental health.
Estrogen receptor modulators are mainly used to treat osteoporosis, which can reduce the probability of fractures in the human body, and they can also improve blood lipids and protect the cardiovascular system. At the same time, it also has certain side effects. For example, this drug has a strong dependence. Once the drug is discontinued, the condition may recur, and it will also affect the cytoskeletal proteins in the central nervous system. The impact on the human body is still relatively large.
Summarize
Selective estrogen receptor modulators (SERMs) are a class of compounds that interact with estrogen receptors in different tissues throughout the body. Their effects vary depending on the tissue and receptor subtype involved. SERMs are used to prevent and treat breast cancer, osteoporosis, and menopausal symptoms. They can inhibit the effects of estrogen on breast tissue, thus slowing down or halting the growth of cancer cells, and provide benefits in treating osteoporosis by reducing the risk of fractures. SERMs are generally well-tolerated, but they can cause side effects. Hormone replacement therapy (HRT) is a treatment option for women experiencing menopausal symptoms, which involves taking estrogen and sometimes progestin. HRT has associated risks, and each woman and her healthcare provider should carefully weigh the risks and benefits. Breast cancer treatment includes surgery, radiation therapy, chemotherapy, targeted therapy, and hormone therapy. The choice of treatment depends on the type, stage, and characteristics of cancer, as well as the patient’s health and preferences.
Conclusion: The Role of SERMs in Medicine
Selective estrogen receptor modulators (SERMs) are versatile drugs that have shown efficacy in treating several medical conditions such as breast cancer, osteoporosis, and menopausal symptoms. By selectively targeting estrogen receptors, SERMs can act as agonists or antagonists depending on the tissue they are targeting, making them unique in their mechanism of action.
However, SERMs have limitations such as the risk of side effects associated with the non-specific activation of estrogen receptors. To address these limitations, ongoing research is focused on developing new SERMs with improved efficacy and reduced side effects. This includes the development of tissue-specific SERMs and more potent drugs with greater selectivity and efficacy.
In conclusion, SERMs have a significant role in the treatment of various medical conditions and will continue to play a role in the future. The development of new and improved SERMs can help overcome the limitations of current SERM therapies, such as nonspecific activation of estrogen receptors, and lead to better patient outcomes and wider medical applications. Continuous research on SERM therapy is likely to lead to further progress and consolidate its important position in medicine. Therefore, SERMs will continue to make important contributions to medical progress and provide valuable treatment options for patients in need.
References
- Jordan, V. C. (2003). Tamoxifen: a most unlikely pioneering medicine. Nature reviews Drug discovery, 2(3), 205-213.
- MILLER, K. E. (2005). Osteoporosis Prevention in Postmenopausal Women. American Family Physician, 72(5), 926-928.
- Jordan, V. C. (2006). Tamoxifen (ICI46, 474) is a targeted therapy to treat and prevent breast cancer. British journal of pharmacology, 147(S1), S269-S276.
- Cummings, S. R., Ettinger, B., Delmas, P. D., Kenemans, P., Stathopoulos, V., Verweij, P., … & Eastell, R. (2008). The effects of tibolone in older postmenopausal women. New England Journal of Medicine, 359(7), 697-708.
- Clarke, B. L., & Khosla, S. (2009). New selective estrogen and androgen receptor modulators. Current opinion in rheumatology, 21(4), 374.
- Yin, D., Gao, W., Kearbey, J. D., Xu, H., Chung, K., He, Y., … & Dalton, J. T. (2003). Pharmacodynamics of selective androgen receptor modulators. Journal of Pharmacology and Experimental Therapeutics, 304(3), 1334-1340.
- Writing Group for the Women’s Health Initiative Investigators, & Writing Group for the Women’s Health Initiative Investigators. (2002). Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. Jama, 288(3), 321-333.
- Pinkerton, J. V. (2020). Hormone therapy for postmenopausal women. New England Journal of Medicine, 382(5), 446-455.
- Burstein, H. J., Lacchetti, C., Anderson, H., Buchholz, T. A., Davidson, N. E., Gelmon, K. A., … & Griggs, J. J. (2019). Adjuvant endocrine therapy for women with hormone receptor-positive breast cancer: ASCO clinical practice guideline focused update. J Clin Oncol, 37(5), 423-438.
- Baselga, J., Campone, M., Piccart, M., Burris III, H. A., Rugo, H. S., Sahmoud, T., … & Hortobagyi, G. N. (2012). Everolimus in postmenopausal hormone–receptor–positive advanced breast cancer. New England Journal of Medicine, 366(6), 520-529.
- Cosman, F., de Beur, S. J., LeBoff, M. S., Lewiecki, E. M., Tanner, B., Randall, S., & Lindsay, R. (2014). Clinician’s guide to prevention and treatment of osteoporosis. Osteoporosis International, 25, 2359-2381.
- Black, D. M., Kelly, M. P., Genant, H. K., Palermo, L., & Eastell, R. (2010). 192. Bucci-Rechtweg C, et al; Fracture Intervention Trial Steering Committee; HORIZON Pivotal Fracture Trial Steering Committee. Bisphosphonates and fractures of the subtrochanteric or diaphyseal femur. N Engl J Med, 362(19), 1761-71.
- Goss, P. E., Ingle, J. N., Alés-Martínez, J. E., Cheung, A. M., Chlebowski, R. T., Wactawski-Wende, J., … & Richardson, H. (2011). Exemestane for breast-cancer prevention in postmenopausal women. New England Journal of Medicine, 364(25), 2381-2391.
- Races, A., & Males, M. W. M. B. (2020). SEER Cancer Statistics Review 1975-2017.
- Early Breast Cancer Trialists’ Collaborative Group. (2011). Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: patient-level meta-analysis of randomized trials. The Lancet, 378(9793), 771-784.
- Jordan, V. C. (2007). SERMs: meeting the promise of multifunctional medicines. Journal of the National Cancer Institute, 99(5), 350-356.
- Jordan, V. C. (2001). Selective estrogen receptor modulation: a personal perspective. Cancer Research, 61(15), 5683-5687.
- Shelly, W., Draper, M. W., Krishnan, V., Wong, M., & Jaffe, R. B. (2008). Selective estrogen receptor modulators: an update on recent clinical findings. Obstetrical & gynecological survey, 63(3), 163-181.
- Patel, H. K., & Bihani, T. (2018). Selective estrogen receptor modulators (SERMs) and selective estrogen receptor degraders (SERDs) in cancer treatment. Pharmacology & therapeutics, 186, 1-24.
- Ferrara, N., & Adamis, A. P. (2016). Ten years of anti-vascular endothelial growth factor therapy. Nature reviews Drug discovery, 15(6), 385-403.
- Cuzick, J., Sestak, I., Cawthorn, S., Hamed, H., Holli, K., Howell, A., & Forbes, J. F. (2015). Tamoxifen for prevention of breast cancer: extended long-term follow-up of the IBIS-I breast cancer prevention trial. The lancet oncology, 16(1), 67-75.